
Prior authorization is the process by which a health insurance plan requires a prescribing provider to obtain approval before a medication will be covered, and for millions of patients, it is the single greatest obstacle standing between a prescription and the pharmacy counter.
Under the pharmacy benefit, prior authorization (PA) touches an enormous share of specialty drugs, creating a layer of administrative review that protects insurers against inappropriate prescribing and that clinicians overwhelmingly describe as a bureaucratic bottleneck built from faxes, hold music, and manual paperwork. The result is delayed therapy, lost prescriptions, and, in many cases, patients who simply give up.
This guide defines exactly what prior authorization is under the pharmacy benefit, maps the specific friction points that turn a routine approval into a weeks-long ordeal, and makes the case, with data, for why automation is no longer a nice-to-have but the only realistic path to making PA immediate and predictable.
Key Takeaways |
|---|
|
What Is Prior Authorization Under the Pharmacy Benefit?
Prior authorization is a utilization management tool used by pharmacy benefit managers (PBMs) and health insurers to control which medications they will cover, and under what conditions. Before dispensing a covered drug, the plan requires the prescriber to submit clinical documentation demonstrating that the medication is medically necessary, that the patient meets specific criteria, and, in many cases, that cheaper alternatives have already been tried and failed.
Under the pharmacy benefit specifically, PA is distinct from medical benefit authorization. It applies to drugs dispensed through retail, mail-order, and specialty pharmacies, and is governed by the formulary rules established by the patient's PBM. This is an important distinction: the payer landscape, the submission channels, and the criteria sets are all different from the medical benefit world, and conflating the two leads to misaligned solutions.
How Prior Authorization Works Step by Step
The PA process follows a predictable, and usually slow, sequence:
Prescriber writes the prescription: The provider submits a new prescription for a formulary drug that requires PA.
Pharmacy flags the PA requirement: The dispensing pharmacy attempts to adjudicate the claim, receives a reject code, and notifies the prescriber's office.
Office staff initiates the PA request: A staff member retrieves the appropriate payer form, collects clinical documentation from the patient's chart, and submits the request.
Payer reviews the submission: The PBM or insurer reviews the clinical evidence against their coverage criteria, a process that can take anywhere from 24 hours to several weeks.
Determination is issued: The payer approves, denies, or requests additional information. Denials trigger the appeals process.
Patient receives (or doesn't receive) their medication: If approved, the prescription is filled. If denied or delayed, the patient waits or walks away.
Each handoff in that sequence is a potential point of failure, and in most practices today, those handoffs are managed by fax, phone, and disconnected payer portals with no shared status visibility.
Which Drugs Typically Require Prior Authorization?
Under the pharmacy benefit, PA requirements are most commonly applied to:
Specialty medications: High-cost biologics, immunotherapies, and rare disease drugs where payers want clinical justification before committing to coverage
Brand-name drugs with generic equivalents: Payers use PA to enforce step therapy, requiring patients to try and fail on a generic before the brand is covered
GLP-1 receptor agonists: Drugs like semaglutide (Wegovy, Ozempic) and tirzepatide (Mounjaro, Zepbound) have become among the most PA-intensive categories as utilization has surged
Controlled substances and select mental health medications: Additional scrutiny is applied to medications with abuse potential or off-label use concerns
Newer market entrants: Drugs recently added to formulary often carry PA requirements while the payer monitors utilization patterns
Payers update their coverage policies regularly, sometimes quarterly, which means a drug that was approved without PA last year may require it today. Office staff relying on institutional memory rather than real-time payer data are perpetually one policy update behind.
Why Prior Authorization Challenges Are Getting Worse
The prior authorization challenges facing providers, patients, and pharma manufacturers today are not new, but they are intensifying. Three converging forces are making the status quo increasingly untenable.
The Volume Problem
The sheer number of PA requests has grown substantially alongside formulary complexity and specialty drug utilization. The AMA's prior authorization research documents year-over-year increases in the percentage of prescriptions requiring PA, with specialty categories seeing the steepest growth. Every new drug launch in a high-scrutiny category (obesity, oncology, immunology) arrives with a PA requirement already attached, and the operational friction that builds up around each request compounds with that volume.
The Payer Complexity Problem
No two payers use the same criteria for the same drug. A GLP-1 agonist PA for a patient on a commercial Blue Cross plan will require different clinical documentation than the same drug for a patient on a regional Medicaid managed care plan. Criteria differ by drug, by plan, by state, and by therapeutic indication.
MGMA's prior authorization landscape research consistently finds that navigating payer-specific criteria is among the top administrative burdens reported by practice managers and that criteria changes arrive faster than staff training cycles can absorb them.
The Technology Gap Problem
Most medical practices and hub service organizations still manage PA using workflows built around fax machines and phone queues. CAQH's annual index of healthcare administrative transactions documents that a substantial share of PA transactions still occur via manual channels, fax and phone, despite the widespread availability of electronic prior authorization (ePA) rails. The gap between what technology can do and what practices actually use is enormous, and patients bear the cost of that gap in delayed therapy starts.
The Bureaucratic Bottlenecks: Where PA Breaks Down
Understanding prior authorization challenges requires going inside the specific friction points where the process loses time, loses information, and loses patients. There are four primary bottlenecks.
Bottleneck 1: The Fax Machine
Fax remains the dominant submission channel for PA requests in many payer-provider relationships. This is documented by CAQH index transaction data and confirmed by virtually every practice operations survey conducted in the past decade.
Fax submission means manual form completion, no submission confirmation, no status tracking, and a process that is entirely dependent on someone at the payer organization physically receiving and routing a piece of paper. Documents get lost. Pages get cut off. Clinical notes fax at unreadable resolution. Each failure restarts the clock.
Bottleneck 2: Phone Queue Hold Times
When office staff need to check PA status, escalate a request, or respond to a payer request for additional information, phone is the primary channel and the time cost is substantial. MGMA's Annual Regulatory Burden Report documents that 60% of practices require at least three employees to complete a single PA request, and 35% report spending more than 35 minutes on average per request. A practice managing dozens of open PA requests at any given time is committing significant hours of staff time per week to a process that is not billable and not clinical.
Bottleneck 3: Disconnected Status Visibility
Once a PA request is submitted, it enters what providers frequently describe as a black hole. There is no shared dashboard, no push notification, no real-time status update accessible to the prescribing practice. The only way to know where a request stands is to call the payer , which returns us to Bottleneck 2. This means patients calling the office for an update get no answer, and prescribers have no visibility into whether a request is pending review, awaiting additional information, or simply lost.
Bottleneck 4: The Appeals Black Hole
When a PA is denied, the appeals process introduces a second layer of bureaucracy on top of the first. Appeal letter generation, clinical documentation assembly, and resubmission are almost entirely manual at most practices.
AMA survey data on prior authorization appeals shows that 67% of physicians who do not appeal denied PAs believe an appeal would be unsuccessful, yet KFF research found that more than 83% of appealed Medicare Advantage denials are eventually overturned. The system is generating enormous administrative waste to arrive at outcomes it would have reached faster with better initial submissions.
What Prior Authorization Delays Cost Patients and Providers
The consequences of prior authorization challenges are not abstract. They manifest as concrete, measurable outcomes across three stakeholder groups.
The Patient Cost: Prescription Abandonment
The most direct patient impact of PA delays is primary non-adherence, patients who receive a prescription but never fill it. Annals of Internal Medicine research on primary non-adherence found that 31.3% of all new prescriptions are never filled, with higher-cost drugs showing the lowest fill rates. For specialty medications and GLP-1 agonists, where PA requirements add both administrative delay and uncertainty about coverage, abandonment rates can be substantially higher and a patient who abandons a prescription during the PA wait is unlikely to return.
The patient experience is straightforward and demoralizing: the pharmacy tells them their medication isn't covered, they wait for the office to sort it out, days pass with no update, they lose confidence in the process, and they stop trying. For patients managing chronic conditions (obesity, diabetes, autoimmune disease) that abandoned prescription is not a minor inconvenience. It is a gap in therapy with real clinical consequences.
The Provider Cost: Administrative Burden and Burnout
The AMA's prior authorization physician survey documents that physicians and their staff spend an average of 13 hours per week on PA-related tasks, nearly two full business days pulled from patient care. The survey also finds that 75% of physicians report that PA denials have risen over the prior five years, and 89% say PA significantly contributes to professional burnout.
For office staff (the medical assistants, nurses, and administrative coordinators who manage the day-to-day PA queue) the burden is even more concentrated. PA management is repetitive, frustrating, and offers no clinical reward. Staff turnover in these roles is high, and institutional knowledge about payer-specific criteria walks out the door with every departure.
The Manufacturer Cost: Lost First Fills and Revenue Leakage
For pharmaceutical manufacturers, particularly those launching specialty drugs or managing established brands in high-PA categories, the PA process represents a direct threat to first-fill rates and patient conversion. When a prescriber writes a prescription and the patient abandons it during the PA wait, that is a lost fill that is unlikely to be recovered.
MGMA's research confirms that 92% of practices have had to dedicate staff resources specifically to PA management, resources that could have gone toward patient care, underscoring how deeply the bottleneck penetrates every layer of the healthcare system, from the practice to the patient to the manufacturer.
Manufacturers invest heavily in hub services and patient support programs to bridge this gap, but traditional hub models that rely on phone-based case management have their own throughput limitations and do not fundamentally solve the bottleneck problem.
Prior Authorization Management: The Traditional Approach and Its Limits
Approach | How It Works | Key Limitation |
In-office PA staff | Dedicated staff manage PA queue manually via fax and phone | High labor cost, limited scalability, staff turnover erodes expertise |
Hub service organizations | Third-party hubs handle PA on behalf of manufacturer programs | Phone-based case management introduces its own delays; limited provider workflow integration |
EHR-embedded ePA | Electronic PA submission via integrated payer rails from within the EHR | Coverage gaps, inconsistent payer adoption, still requires manual form-filling |
Payer portal submission | Staff submit PAs through individual payer web portals | Requires separate logins per payer, no consolidated status view, high staff time cost |
Standalone PA software | Dedicated PA management tools outside clinical workflow | Requires behavior change from providers; adoption is typically low |
Electronic submission via ePA rails is better than fax, but it still requires staff to find the right form, populate it correctly, and monitor a separate system for status updates. Payer portals consolidate submission but fragment visibility. Hub services add human capacity but not speed.
The common thread across every traditional approach is that they digitize the existing process rather than eliminating the manual steps that make it slow. This is where the gap between traditional PA management and modern automation is most stark and most consequential for patients.
Why Automation Is the Necessary Path Forward for PA for Medication
The good news is that the technology required to solve prior authorization challenges at the root is not theoretical. GenAI-native platforms that combine real-time benefit verification, intelligent PA form completion, multi-channel submission, and proactive determination follow-up are operational today and the results they are delivering are not incremental improvements. They are step-change reductions in time-to-therapy.
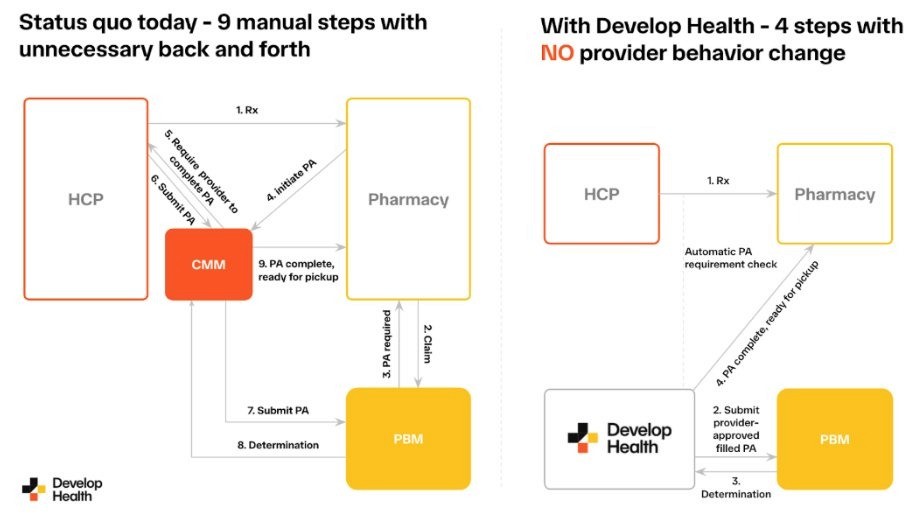
The diagram below shows the difference between a manual PA process and a fully automated PA process. The manual PA workflow requires 9 steps and constant back-and-forth between the HCP, pharmacy, and PBM. With genuine automation, that collapses to 4 steps, with no behavior change required from the provider.
What Genuine PA Automation Looks Like
Genuine automation for PA for medication does not mean a better fax-to-email gateway or a portal with a slightly faster login. It means:
Automated benefit verification (BV) at the point of prescribing: Before a prescription is even written, the system checks the patient's coverage, confirms whether PA is required, and surfaces out-of-pocket cost estimates inline in the provider's EHR. No phone call, no separate lookup.
AI-powered form completion: When PA is required, the system extracts relevant clinical evidence from the patient's chart using OCR and large language models, pre-populates the payer-specific PA form with citations to supporting documentation, and flags gaps before submission.
Multi-channel submission with intelligent routing: The system submits via ePA rails where available, falls back to AI-assisted fax or phone where not, and maintains a complete audit trail regardless of channel.
Proactive determination follow-up: Rather than waiting for the payer to respond, the system actively monitors status, follows up on pending requests, and routes determinations back to the prescriber through the EHR task queue.
Denial intelligence and appeals automation: When a denial is issued, the system analyzes the denial reason, generates a tailored appeal letter using clinical evidence from the chart, and initiates resubmission, all without requiring staff to start from scratch.
The Evidence for Automation's Impact
This is not aspirational technology. Platforms operating at scale today are delivering measurable results that validate the automation-first approach. Here are a few insights from Develop Health’s customer base:
Approval cycle time reduced from 1.5 weeks to 20 hours: One customer moved their prescription-to-approval cycle from a week and a half down to under a day by replacing manual hub workflows with Gen AI-native automation.
83% reduction in PA handling time: Develop Health has delivered an 83% reduction in the time staff spend on PA management per request, not by adding more people to the process, but by removing the manual steps that consumed staff hours.
14% boost in approval rates: By improving the quality of initial submissions (better evidence extraction, better form completion, better payer-specific optimization) Develop Health is achieving higher approval rates on first submission, reducing the volume of denials that require costly appeals.
Why Provider-First Design Matters
One of the most persistent failure modes in PA technology is solutions that require providers to change their behavior: to log into a new portal, to learn a new interface, to add a new step to their workflow. Adoption collapses when the tool adds friction rather than removing it.
The most effective automation platforms are designed to be invisible to the provider. They embed directly into the EHR workflow, surface PA information in the task queue the provider already uses, and require no application-hopping or behavior change from clinical staff. This is the difference between a tool that gets adopted and a tool that gathers dust.
MGMA's documented findings on PA administrative burden make clear why low-friction integration is essential: 92% of practices have already had to hire or reassign staff just to handle PA volume, meaning any solution that adds steps rather than removes them simply compounds an already critical problem. The right approach also depends on which EHR a practice uses, the PA tooling landscape inside athenahealth, for example, has its own set of native and third-party options, and the same is true for large health systems running Oracle Health (Cerner) Millennium.
Common Prior Authorization Mistakes and How Automation Fixes Them
Mistake 1: Submitting Without Verifying PA Requirements First
The single most common avoidable PA delay is submitting a prescription for a drug that requires PA without knowing it in advance. The office learns about the requirement only when the pharmacy rejects the claim, at which point the patient is already at the counter expecting their medication.
How automation fixes it: Real-time benefit verification at the point of prescribing surfaces PA requirements before the prescription is written. The provider knows, the patient is counseled, and the PA process begins immediately rather than after a pharmacy rejection.
Mistake 2: Submitting Incomplete Clinical Documentation
Payers deny a significant percentage of PA requests on the first submission due to missing or insufficient clinical documentation. The criteria for a given drug on a given plan are specific, they may require documented BMI thresholds, prior therapy attempts, comorbidity evidence, or lab values, and a submission that does not speak directly to those criteria will be denied, adding days or weeks to the process.
How automation fixes it: AI-powered form completion extracts the specific clinical evidence required by each payer's criteria set and populates the form with citations to the chart. The gap between what the payer needs and what was submitted shrinks to near-zero.
Mistake 3: Passive Status Monitoring
Most PA processes rely on the payer to notify the practice of a determination. In reality, determinations are frequently made without timely notification, requests sit in review queues past their deadlines, and practices have no visibility into status until they initiate an outbound call.
How automation fixes it: Automated status monitoring and proactive payer follow-up ensures that pending requests are never simply waiting; the system actively tracks and escalates, and determinations route back to the practice immediately rather than sitting in a fax inbox.
Mistake 4: Abandoning Denied PAs Without Appeal
AMA data on prior authorization outcomes shows that a significant proportion of initial PA denials are overturned on appeal, but most practices appeal only a fraction of denials, because the appeal process is manual, time-consuming, and deprioritized relative to the ongoing PA queue. The result is that clinically appropriate medications are permanently denied not because the payer was right, but because the practice ran out of bandwidth to fight.
How automation fixes it: Denial analysis and appeal automation generate tailored appeal letters using the specific denial reason code and relevant clinical evidence from the char, when appropriate. Appeals are submitted automatically, and resubmission rates increase without adding to staff workload.
The Future of Prior Authorization: What Reform and Technology Mean for Medication Access
The prior authorization landscape is changing on two fronts simultaneously: regulatory reform and technological disruption. Understanding both is essential for anyone managing PA programs at scale.
Regulatory Reform: CMS and the Push for Transparency
CMS's interoperability and prior authorization final rule represents the most significant federal action on PA reform in recent years. The rule requires payers to implement electronic prior authorization, to provide specific reasons for PA denials, and to reduce PA decision timelines. While implementation timelines are phased and enforcement remains an open question, the regulatory direction is clear: the federal government has identified PA as a patient access problem and is applying structural pressure on payers to modernize.
While implementation timelines are phased and enforcement remains an open question, the regulatory direction is clear: the federal government has identified PA as a patient access problem and is applying structural pressure on payers to modernize. The convergence of the IRA, MFN price negotiations, and CMS-0057-F is reshaping payer behavior and PA complexity in ways access teams need to understand in detail.
Step Therapy Reform at the State Level
Dozens of states have enacted or are considering step therapy reform legislation, which limits payers' ability to require patients to try and fail on alternative medications before accessing the prescribed drug. The National Alliance of Mental Illness and similar patient advocacy organizations have been active in advocating for these protections, particularly in mental health and chronic disease categories. Step therapy restrictions do not eliminate PA, but they limit one of its most clinically contested applications.
What This Means for Automation Strategy
Regulatory reform and technology are not substitutes for each other — they are complements. Even as CMS and state legislatures push payers toward faster, more transparent PA processes, the volume of PA requests is not going to decrease meaningfully in the near term. The clinical complexity of specialty drug categories is increasing, not decreasing. The operational answer is automation that is designed to adapt to changing payer requirements, platforms that update criteria sets and submission pathways continuously, so that a change in payer policy does not require a corresponding change in staff training.
Frequently Asked Questions
What is prior authorization under the pharmacy benefit?
Prior authorization under the pharmacy benefit is a process by which a health insurer or PBM requires a prescriber to obtain approval before a medication will be covered and dispensed. It applies to drugs filled at retail, mail-order, and specialty pharmacies, and is governed by the formulary rules and coverage criteria of the patient's pharmacy benefit plan. PA under the pharmacy benefit is distinct from medical benefit authorization, which applies to drugs administered in a clinical setting.
How long does prior authorization take?
Under current manual and semi-manual workflows, PA under the pharmacy benefit can take anywhere from 24 hours to two weeks or more, depending on the payer, the drug category, and the completeness of the initial submission. AMA prior authorization research documents that delays of multiple days are common, and that urgent requests are not reliably expedited. With automation, platforms like Develop Health are reducing approval cycle times to under 24 hours for the majority of requests.
Why do insurance companies require prior authorization?
Insurers and PBMs use prior authorization as a utilization management tool, to ensure that high-cost medications are being prescribed for appropriate indications, that step therapy protocols have been followed, and that the medication is medically necessary for the specific patient. In theory, PA controls costs and ensures appropriate use. In practice, the AMA and MGMA document that PA criteria frequently function as administrative barriers rather than meaningful clinical filters, and that the process imposes costs on the healthcare system that exceed its clinical benefits.
What happens if prior authorization is denied?
If a PA is denied, the prescriber has the right to appeal the decision. The appeals process requires submitting additional clinical documentation, a letter of medical necessity, and in some cases a peer-to-peer review between the prescribing physician and a payer medical director. AMA data on PA outcomes shows that a substantial percentage of initial denials are overturned on appeal, but the appeals process is time-consuming, and many practices lack the bandwidth to pursue all eligible appeals.
What is the difference between prior authorization and step therapy?
Prior authorization is a broad category of payer approval requirements. Step therapy is a specific type of PA criterion that requires a patient to try and fail on one or more alternative (typically lower-cost) medications before the requested drug will be covered. Step therapy is most common in chronic disease categories (including mental health, autoimmune disease, and obesity) and is a frequent source of clinical controversy, as it can override a prescriber's clinical judgment about the most appropriate first-line treatment.
How can prior authorization management be improved at the practice level?
The most impactful improvements to PA management come from three areas:
implementing real-time benefit verification so that PA requirements are known before the prescription is written
moving from manual fax-and-phone submission to electronic prior authorization (ePA) wherever possible
adopting platforms that automate status monitoring and denial appeals rather than relying on staff to manage these tasks reactively.
For practices and hub service organizations managing high volumes of PA, GenAI-native automation platforms that embed directly into EHR workflows offer the most significant time-to-therapy improvements currently available.
AMA: Prior Authorization Research Reports: physician survey data on PA burden, delay frequency, and burnout impact. https://www.ama-assn.org/practice-management/prior-authorization/prior-authorization-research-reports
CAQH: CAQH Index Report: annual benchmarking of healthcare administrative transactions including PA volume and channel mix. https://www.caqh.org/insights/caqh-index-report
Annals of Internal Medicine: Primary Non-Adherence to Prescribed Medications: evidence on the relationship between access friction and prescription abandonment. https://www.acpjournals.org/doi/10.7326/M13-1705
MGMA: The Prior Authorization Landscape in 2025: practice manager survey data on administrative burden and PA volume growth. https://www.mgma.com/articles/the-prior-authorization-landscape-in-2025
CMS: CMS Finalizes Rule to Expand Access to Health Information and Improve the Prior Authorization Process: summary of the CMS interoperability and prior authorization final rule. https://www.cms.gov/newsroom/press-releases/cms-finalizes-rule-expand-access-health-information-and-improve-prior-authorization-process
NAMI: National Alliance on Mental Illness: patient advocacy resources on step therapy reform and PA impact on mental health medication access. https://www.nami.org
KFF: Medicare Advantage Insurers Made Nearly 53 Million Prior Authorization Determinations in 2024 https://www.kff.org/medicare/medicare-advantage-insurers-made-nearly-53-million-prior-authorization-determinations-in-2024/








